
The Latest Research on Perimenopause Symptoms Will Surprise You
I have a PhD and 20 yrs of clinical experience. Perimenopause still caught me off guard! Here's what I've learned.
For me, perimenopause symptoms started at 40. The intense pain in my feet was like I was walking on nails. Then my knees started cracking every time I climbed a flight of stairs. Last, came the deep ache in my hips. Yet every time I went to a doctor, they would look at my labs and imaging and the answer would come back the same: "Everything looks normal."
For those of us in the perimenopause years, normal is a complicated word. Normal means the pain is real but nothing is showing up on the x-ray or MRI. It means you leave the appointment with no solutions, just a referral to yet another specialist. Or even worse, a narrative that the pain is all in your head.
As a clinical educator and an avid researcher, I can assure you that pain and the many other symptoms that can come with perimenopause are very real. But even with all my education and experience as a clinician, it took me years, numerous labs, and countless research hours to gain the language I needed to discuss my experience with doctors.
I wrote this article so you don't have to wait as long as I did — or work as hard — to get the care you need.
1. Perimenopause, not menopause, is the big transition
Perimenopause typically begins in the early to mid-40s, sometimes even the late 30s, and lasts on average 4 to 8 years (Wegrzynowicz et al., 2025). Clinically, perimenopause starts with the onset of irregular periods. It finally ends after 12 consecutive months without a menstrual cycle, which is the point that officially marks menopause (Yang et al., 2024).
Perimenopause typically begins in the early to mid-40s, sometimes even the late 30s, and lasts on average 4 to 8 years. Clinically, perimenopause starts with the onset of irregular periods. It finally ends after 12 consecutive months without a menstrual cycle, which is the point that officially marks menopause.
So menopause is actually a single point in time that is identified only after it's happened. Perimenopause is the actual struggle—when many of us face an unpredictable onslaught of whole-body symptoms.
The Many Symptoms of Perimenopause
According to the NHS, any of the following symptoms can accompany perimenopause and last 7-9 years. Severity and duration vary from one person to the next. Certain symptoms, like hot flushes have been found to disproportionally impact Black women.
- Bone density loss/osteoporosis risk
- Dry/itchy skin
- Hair thinning or loss
- Headaches and migraines
- Hot flushes and night sweats
- Irregular periods
- Mood changes
- Muscle aches and joint pain
- Painful sex
- Palpitations
- Poor memory and brain fog
- Reduced libido
- Sensitive teeth, painful gums
- Sleep problems
- Urinary incontinence or urgency
- UTIs or UTI-like symptoms
- Vaginal dryness/burning/irritation
- Weight gain
2. Fluctuating estrogen — not low estrogen — drives perimenopause symptoms
Despite what you may have read or heard, the defining feature of perimenopause is not low estrogen, it's fluctuating estrogen. Estrogen levels during perimenopause do not steadily decline. They rise and fall like a rollercoaster, sometimes spiking higher than normal before crashing (Harvard Health, 2022; Santoro, 2016; Grub et al., 2021).
And because estrogen receptors are spread out throughout the entire body, not just in the reproductive system, fluctuating levels can cause symptoms across every organ system, affecting the brain, heart, joints, muscles, bladder, skin, and hair (Yang et al., 2024; UCLA Health, 2025).
💡 Stop and reflect: When you think about the dramatic shifts in your mood recently, have you attributed them to parenting stress, work pressure, or feeling out of sync with your partner?
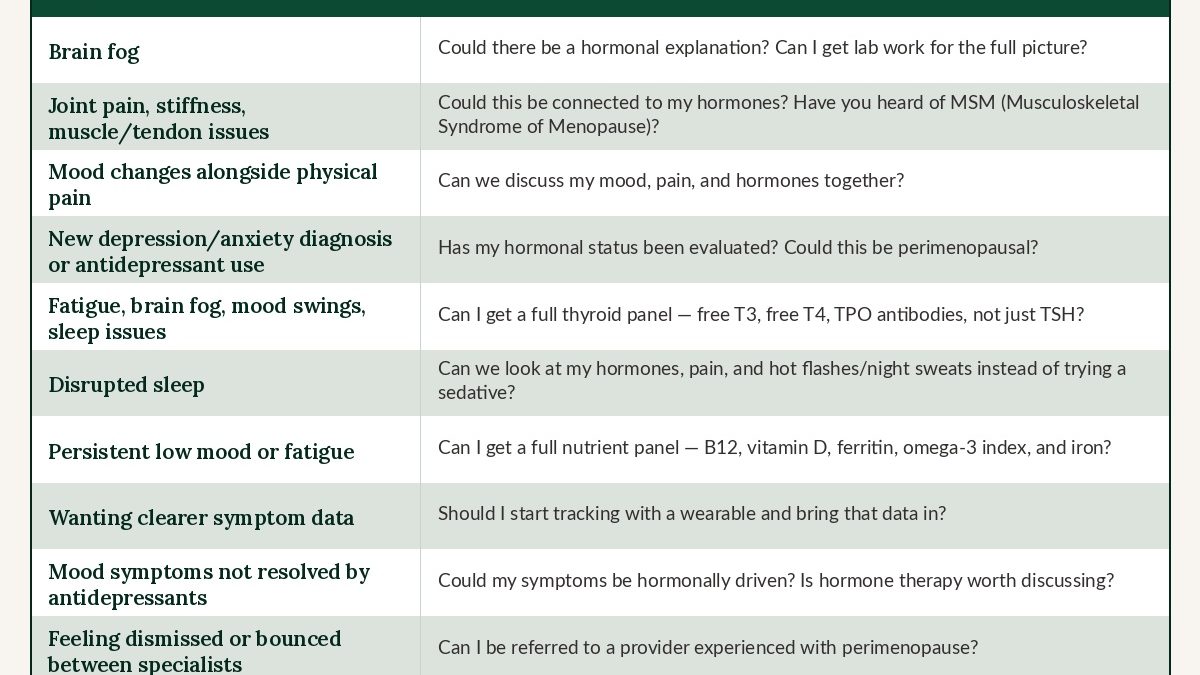
Those things may be real, but there is also a measurable, hormonal explanation worth looking into. You probably do not have lab work that shows you the full picture yet. Now might be the time to request it.
3. Perimenopause “brain fog” is more serious than you might think
Estrogen receptors are distributed throughout the brain, and many of the complaints that prompt women to seek mental health treatment during perimenopause can be traced back to fluctuating hormones (Mosconi et al., 2024).
Researchers who have studied women in perimenopause have reported measurable changes in brain structure, connectivity, and energy metabolism throughout the transition (Mosconi et al., 2024). It's no wonder we can't think straight!
4. Perimenopause joint pain is real — and finally has a name
Estrogen receptors are present throughout joints, tendons, cartilage, skeletal muscle, and bone. As estrogen declines during the perimenopausal transition, it can lead to all of the following:
- Widespread joint pain
- Accelerated muscle and strength loss
- Increased tendon vulnerability
- Cartilage degradation
- Progression of osteoarthritis
Up to 71% of perimenopausal women experience these symptoms, and up to 25% will be disabled by them at some point during the perimenopause transition (Wright et al., 2024).
In October 2024, researchers published a clinical review that officially gave a name to these collective effects: the Musculoskeletal Syndrome of Menopause (MSM) (Wright et al., 2024).
💡 Stop and reflect: What pain has come up for you that feels invisible? Has anyone in a medical appointment ever connected that pain to your hormones? Now you have the language to ask and this study to share.
5. Perimenopause mood changes and pain make each other worse
Mood problems and pain can not only co-exist, they both amplify and fuel each other.
Research shows that (Salas-Gonzáles et al., 2025):
- Chronic pain increases anxiety and depression
- Anxiety lowers pain thresholds and heightens sensitivity
- Depression increases how intensely people perceive pain
Given that, it makes sense that the prevalence of depression and anxiety among adults with chronic pain is approximately 40% — significantly higher than in comparison groups (Aaron et al., 2025).
Perimenopause mood issues and pain can also be due to something called allostatic load. Basically, your body has a measurable tolerance for how much stress it can take before systems start to break down. When you're in your late 30s or 40s, things like long work days, active parenting, chronic pain, and financial strain can push you over the edge.
Research shows that chronic stress and high allostatic load are among the strongest risk factors for mood disorders during perimenopause, independent of hormonal levels alone (McElhany et al., 2024).
Clinicians often overlook allostatic load when diagnosing generalized anxiety disorder, major depressive episode, fibromyalgia, or somatization in perimenopausal women.
💡 Stop and reflect: Have you received a new depression or anxiety diagnosis in your 40s that you never had before? Has anyone had a conversation with you that connected your mood, your pain, and your hormonal status in the same appointment? If not, that conversation is overdue.
6. Antidepressants are overprescribed during perimenopause
Research has found that women ages 45 to 54 going through perimenopause experienced higher rates of common mental health diagnoses than men in the same age group. Women in this group were also prescribed more SSRIs and SNRIs than similar-aged men with the same diagnoses (Alsugeir et al., 2024).
At the same time, use of Menopausal Hormone Therapy (MHT) among US postmenopausal women dropped from 26.9% in 1999 to just 4.7% by 2020 due to a misrepresentation of findings in the Women's Health Initiative (WHI)'s 2002 study (Yang et al., 2024).
The result is that women have been heavily medicated for mood and chronically undertreated hormonally.
On the bright side, new guidelines make it clear that clinicians must identify women's menopausal stage and assess co-occurring hormonal symptoms before diagnosis and treatment (Maki et al., 2019). When hormonal symptoms are overlooked, treatments may provide partial relief, enough to feel helpful, but not enough to address the root cause of symptoms (Mogallapu et al., 2025).
💡 Stop and reflect: Before you fill the next prescription, ask: Has anyone evaluated my hormonal status? Could what I am experiencing be perimenopausal in origin? Don't hesitate to ask for additional testing.
7. Thyroid problems are harder to diagnose in perimenopause
Subclinical hypothyroidism, a condition where TSH (Thyroid Stimulating Hormone) is mildly elevated but thyroid hormone levels appear normal, affects an estimated 6 to 10% of women during their reproductive years (Mintziori et al., 2024).
The symptoms, which include fatigue, cognitive impairment, mood lability, and sleep disturbance, overlap so significantly with perimenopausal depression that the two are difficult to distinguish without more complete testing (Lang et al., 2025).
A TSH value is a starting point, but including free T3, free T4, and TPO antibodies in lab testing tells a more complete story. If you are experiencing the symptoms listed above and have not found relief with standard treatment, ask if you can get a full thyroid panel.
💡 Stop and reflect: Has anyone suggested you do a full thyroid panel rather than just TSH? If not, it's time to be thorough; add it to your list of questions for the next appointment.
8. Sedatives won’t work for perimenopause sleep disruption
If you're in the age range for perimenopause, it's critical to consider hormones when evaluating sleep disturbance (aka you wake up after you've fallen asleep). Fluctuations in estrogen and progesterone directly affect sleep quality, while vasomotor symptoms (hot flashes and night sweats) are documented contributors to nocturnal awakenings (Lang et al., 2025; Troìa et al., 2025).
What's happening in a nutshell: Your hormones are erratic, your body temperature is dysregulating in the middle of the night, and that is likely what's waking you up.
Research findings also show that abnormal sleep in perimenopausal women — specifically lower sleep efficiency (how long you're in bed vs. how long you're asleep), increased wakefulness after sleep onset, and reduced REM sleep — are significantly associated with higher cortisol levels, which isn't the case for self-reported insomnia and sleepiness outside of perimenopause (Sahola et al., 2024).
This cortisol link is a vicious cycle: It's caused by poor sleep AND it actively prevents deeper, restorative REM sleep from happening. Taking sedatives will not break this cycle.
For women also experiencing MSM, sleep disruption is also frequently pain-driven, and co-existing musculoskeletal disorders are documented contributors to sleep disturbance alongside vasomotor and mood symptoms (Troìa et al., 2025).
💡 Stop and reflect: If you have been offered sedative sleep medication without anyone asking about your hormone levels, your pain, or whether you are waking up hot, you need a more complete assessment.
9. Vitamin deficiencies in perimenopause can mimic mood disorders
Although doctors seldom mention it in routine appointments, women in perimenopause are at significantly increased risk of deficiencies in specific vitamins and nutrients. And those deficiencies can produce symptoms that look nearly identical to a mood disorder (Wylenzek et al., 2024).
- Low vitamin B6 is linked to cognitive decline, and mood disruption.
- Low vitamin B12 is associated with depression, cognitive impairment, and increased dementia risk.
- Vitamin D deficiency presents as fatigue, mood instability, immune dysregulation, and bone loss.
- Iron deficiency, which can accelerate during perimenopause when cycles become irregular and heavier before stopping, contributes directly to fatigue, brain fog, and low mood.
- Omega-3 fatty acids, which most of us are not consuming at adequate levels through diet alone, are linked to vasomotor symptom management, mood regulation, and sleep quality.
💡 Stop and reflect: Has anyone run a full nutrient panel for you recently (this means looking at B12, vitamin D, ferritin, omega-3 index, and iron)? If not, add those to the list for your next appointment.
10. Wearable devices can help track perimenopause symptoms
Consumer wearable devices like an Apple Watch, Oura Ring, WHOOP, or Garmin provide long-term continuous monitoring across sleep, rest, and activity. This data can provide a clinician with a helpful, longer-term picture of what's happening with your body (Li et al., 2023).
One thing to look for is heart rate variability (HRV), which is measurably decreased during perimenopause. Lower HRV correlates with more perimenopause symptoms (Martinelli et al., 2020).
💡 Stop and reflect: Do you currently have a wearable? Start tracking now. The data you collect may be the most useful thing you bring to your next appointment.
11. HRT can significantly improve mood in perimenopause
Research shows that for women whose depression and anxiety started during perimenopause (particularly those without a significant psychiatric history), antidepressant treatment alone is incomplete (Mogallapu et al., 2025; Glynne et al., 2025).
Adding HRT can help. A study assessing the impact of transdermal estradiol (aka an estrogen patch) — with or without progesterone and testosterone — on mood symptoms in 920 peri- and postmenopausal women, found significant improvements across mood-related symptoms, with additional benefit in women who received both estradiol and testosterone (Glynne et al., 2025).
💡 Stop and reflect: Has anyone ever asked whether your mood symptoms might be hormonally driven? Has the word estradiol ever come up in a mental health conversation? If not bring it up with your medical provider.
12. The right medical team makes all the difference
Women in perimenopause are routinely undertreated for a host of reasons:
- Symptoms are distributed across the entire body
- Imaging is often normal
- The clinical picture does not fit neatly into any single specialty's lane
- Most providers have not been trained to assess hormonal patterns
So if you're experiencing symptoms that non-hormonal treatments aren't fully addressing, it's worth finding both mental health and medical providers with a passion for perimenopause.
Medical providers can include a primary care provider, an endocrinologist, and a gynecologist.
Counseling is also essential (Lang et al., 2025). A good mental health provider who understands this landscape can help you build language for medical conversations, process the grief of a body that is changing without warning, and hold the emotional weight while the medical picture gets sorted.
One last fact: perimenopause care isn’t equally available to everyone
Access to hormonal evaluation, specialist care, and emerging options (like medical cannabis for pain) is not equally distributed across income, geography, or race. For example, it's well documented that Black women's concerns are dismissed more frequently compared to White women (Agarwal et al., 2024).
If you have encountered barriers, delays, or dismissals, that experience reflects a systemic issue, not the validity of your symptoms. Keep advocating!
Bring this article, bring your data, and find a provider who speaks this language, because you deserve a complete assessment and informed treatment. The pain that I started feeling at 40 was not stress, it was not anxiety, and it was not just getting older; it was hormonal, and it had a name all along.
Take action:
Protect your mental health in perimenopause
Dealing with the stress of perimenopause symptoms and the challenge of finding medical care is far more manageable with a expert therapist in your corner. At Alma, we make it easy to get started with a licensed clinician who specializes in women’s mental health and accepts your insurance.
ABOUT THE AUTHOR
Jill M. Krahwinkel-Bower, PhD, has been a Counselor Educator since 2014 and is currently an Assistant Professor at Kutztown University. She has been counseling since 2006 with a variety of clinical experience working with adults, adolescents, children, and families on needs related to depression, anxiety, trauma, bereavement, adjustment, relationships, self-esteem, wellness management, substance use, and more. She offers a culturally responsive, social justice-oriented approach that concentrates on meeting the needs of LGBTQ+, Black, Indigenous, and People of Color (BIPOC).
DR. Krahwinkel-Bower also provides clinical supervision for master-level intern students and graduates working towards their licensure as professional counselors. She advocates at the state and national level, attends and presents at regional and national conferences, and volunteers in her local community.
References:
Aaron, R. V., Ravyts, S. G., Carnahan, N. D., Bhattiprolu, K., Harte, N., McCaulley, C. C., Vitalicia, L., Rogers, A. B., Wegener, S. T., & Dudeney, J. (2025). Prevalence of depression and anxiety among adults with chronic pain: A systematic review and meta-analysis. JAMA Network Open, 8(3), Article e250268. Link
Agarwal, A. K., Gonzales, R. E., Sagan, C., Nijim, S., Asch, D. A., Merchant, R. M., & South, E. C. (2024). Perspectives of Black patients on racism within emergency care. JAMA Health Forum, 5(3), Article e240046. Link
Alsugeir, D., Adesuyan, M., Talaulikar, V., Wei, L., Whittlesea, C., & Brauer, R. (2024). Common mental health diagnoses arising from or coinciding with menopausal transition and prescribing of SSRIs/SNRIs medications and other psychotropic medications. Journal of Affective Disorders, 364, 259–265. Link
Glynne, S., Kamal, A., McColl, L., Newson, L., Reisel, D., Mu, E., Hendriks, O., Saini, P., Gurvich, C., & Kulkarni, J. (2025). Transdermal oestradiol and testosterone therapy for menopausal depression and mood symptoms: Retrospective cohort study. The British Journal of Psychiatry. Advance online publication. Link
Grub, J., Süss, H., Willi, J., & Ehlert, U. (2021). Steroid hormone secretion over the course of the perimenopause: Findings from the Swiss Perimenopause Study. Frontiers in Global Women's Health, 2, Article 774308. Link
Harvard Health Publishing. (2022, August). Perimenopause: Rocky road to menopause. Harvard Health. Link
Lang, X.-L., Huang, C.-C., Cui, H.-Y., Zhong, H.-X., Shen, M.-Y., & Zhao, F. (2025). From physiology to psychology: An integrative review of menopausal syndrome. World Journal of Psychiatry, 15(11), Article 108713. Link
Li, K., Cardoso, C., Moctezuma-Ramirez, A., Elgalad, A., & Perin, E. (2023). Heart rate variability measurement through a smart wearable device: Another breakthrough for personal health monitoring? International Journal of Environmental Research and Public Health, 20(24), Article 7146. Link
Maki, P. M., Kornstein, S. G., Joffe, H., Bromberger, J. T., Freeman, E. W., Athappilly, G., Bobo, W. V., Rubin, L. H., Koleva, H. K., Cohen, L. S., & Soares, C. N. (2019). Guidelines for the evaluation and treatment of perimenopausal depression: Summary and recommendations. Journal of Women's Health, 28(2), 117–134. Link
Martinelli, P. M., Sorpreso, I. C. E., Raimundo, R. D., Junior, O. D. S. L., Zangirolami-Raimundo, J., Malveira de Lima, M. V., Pérez-Riera, A., Pereira, V. X., Elmusharaf, K., Valenti, V. E., & de Abreu, L. C. (2020). Correction: Heart rate variability helps to distinguish the intensity of menopausal symptoms: A prospective, observational and transversal study. PLOS ONE, 15(2), Article e0229094. Link
McElhany, K., Aggarwal, S., Wood, G., & Beauchamp, J. (2024). Protective and harmful social and psychological factors associated with mood and anxiety disorders in perimenopausal women: A narrative review. Maturitas, 190, Article 108118. Link
Mintziori, G., Veneti, S., Poppe, K., Goulis, D. G., Armeni, E., Erel, C. T., Fistonić, I., Hillard, T., Lindén Hirschberg, A., Meczekalski, B., Mendoza, N., Mueck, A. O., Simoncini, T., Stute, P., van Dijken, D., Rees, M., Duntas, L., & Lambrinoudaki, I. (2024). EMAS position statement: Thyroid disease and menopause. Maturitas, 185, Article 107991. Link
Mogallapu, R., Sarich, R., Chalia, A., Ang-Rabanes, M., Gibson, E., Sugnanam, V., & Vudathaneni, V. K. P. (2025). Beyond selective serotonin reuptake inhibitor (SSRIs): Exploring hormonal therapy for mood disorders in perimenopause and postmenopause. Cureus, 17(10), Article e94752. Link
Mosconi, L., Berti, V., Dyke, J., Schelbaum, E., Jett, S., Loughlin, L., Jang, G., Rahman, A., Hristov, H., Pahlajani, S., Andrews, R., Matthews, D., Etingin, O., Ganzer, C., de Leon, M., Isaacson, R., & Brinton, R. D. (2021). Menopause impacts human brain structure, connectivity, energy metabolism, and amyloid-beta deposition. Scientific Reports, 11, Article 10867. Link
Mosconi, L., Nerattini, M., Matthews, D. C., Jett, S., Andy, C., Zarate, C., Carlton, C., Kodancha, V., Schelbaum, E., Williams, S., Pahlajani, S., Loeb-Zeitlin, S., Havryliuk, Y., Andrews, R., Pupi, A., Ballon, D., Kelly, J., Osborne, J., Nehmeh, S., Fink, M., Berti, V., Matthews, D., Dyke, J., & Brinton, R. D. (2024). In vivo brain estrogen receptor density by neuroendocrine aging and relationships with cognition and symptomatology. Scientific Reports, 14, 12680. Link
Sahola, N., Toffol, E., Kalleinen, N., & Polo-Kantola, P. (2024). Worse sleep architecture but not self-reported insomnia and sleepiness is associated with higher cortisol levels in menopausal women. Maturitas, 187, Article 108053. Link
Salas-González, J., Heredia-Rizo, A. M., Fricke-Comellas, H., Chimenti, R. L., & Casuso-Holgado, M. J. (2025). Patterns of pain perception in individuals with anxiety or depressive disorders: A systematic review and meta-analysis of experimental pain research. The Journal of Pain, 35, Article 105530. Link
Santoro, N. (2016). Perimenopause: From research to practice. Journal of Women's Health, 25(4), 332–339. Link
Troìa, L., Garassino, M., Volpicelli, A. I., Fornara, A., Libretti, A., Surico, D., & Remorgida, V. (2025). Sleep disturbance and perimenopause: A narrative review. Journal of Clinical Medicine, 14(5), Article 1479. Link
UCLA Health. (2025, February). Sneaky symptoms of perimenopause. UCLA Health News. Link
Wegrzynowicz, A. K., Walls, A. C., Godfrey, M., & Beckley, A. (2025). Insights into perimenopause: A survey of perceptions, opinions on treatment, and potential approaches. Women, 5(1), Article 4. Link
Wright, V. J., Schwartzman, J. D., Itinoche, R., & Wittstein, J. (2024). The musculoskeletal syndrome of menopause. Climacteric, 27(5), 466–472. Link
Wylenzek, F., Bühling, K. J., & Laakmann, E. (2024). A systematic review on the impact of nutrition and possible supplementation on the deficiency of vitamin complexes, iron, omega-3 fatty acids, and lycopene in relation to increased morbidity in women after menopause. Archives of Gynecology and Obstetrics, 310(4), 2235–2245. Link
Yang, J. L., Hodara, E., Sriprasert, I., Shoupe, D., & Stanczyk, F. Z. (2024). Estrogen deficiency in the menopause and the role of hormone therapy: Integrating the findings of basic science research with clinical trials. Menopause, 31(10), 926–939. Link
Yang, L., Toriola, A. T. (2024). Menopausal hormone therapy use among postmenopausal women. JAMA Health Forum, 5(9), Article e243128. Link
Related Articles



Apr 7, 2026

Looking for a therapist?
Get tips on finding a therapist who gets you.
By subscribing to emails from Alma, you are agreeing to Alma's privacy policy.